Your attachment profile depends on experiences around your birth and infant years and the relationship with your primary care giver.
Maternal deprivation theory
John Bowlby (1907 – 1990) was a psychoanalyst who came up with the maternal deprivation theory which basically linked adult mental health with maternal attachments/separations or detachments in the child’s early life.
Bowlby’s basic theory in a nutshell:
- A child needs to attach to a main attachment figure usually the mother (monotropy);
- This main attachment figure should be the one caring for the child’s first 2 years of life;
- If this does not occur and there are separations from the attachment figure, then the long- term consequences will include problems for the child later in life including:
- Developmental problems with intellect
- Psychopathy lacking affection/empathy
- Aggression
- The stages of distress an infant reaches when separated from the primary caregiver starts with protest-(usually crying out), then leads to despair-(inconsolable even if others try to comfort the child), and finally detachment-(if the separation continues the child may or may not engage with others, but will reject the main caregiver and show strong signs of anger).
Bowlby concluded that maternal separation/deprivation in the child’s early life caused permanent emotional damage.

Attachment theory – pre birth
Other experts developed similar theories more recently now known as attachment theory . This also includes how a mother’s trauma during pregnancy can affect the mental condition of the baby prior to being born, because of cortisol passing through the placenta affects the baby’s development. In other words the mother’s dysregulated state is passed onto the baby.
Secure Attachment
After the baby is born and grows to be a toddler he/she will expect his/her main attachment caregiver to be there whilst he/she moves around and explores, crawls etc and if that is the case he/she will feel secure and safe and comfortable exploring and have a “secure attachment” .
When the infant then becomes a toddler, and has a secure base or secure attachment figure, he/she can then explore. Because he/sh knows that secure base is going to be there and he/she can come back to that secure base and he/she can come back to that secure base.
Natural development instigated by curiosity, exploration of motor skills and socializing will help develop the baby’s mental and social skills as it is actively exploring.
Insecure Attachment
On the other hand. if a young child did not have a secure attachment or was physically or sexually abused or grossly neglected, that trauma will make the child focus on fear and survival. This can lead to all sorts of issues later in life including becoming unnecessarily hyper vigilant almost as part of their personality.
That is their main focus rather than enjoying exploration- they have only safety high on their radar. Basically they are hard wired to seek out danger more than other people.
Types of insecure attachments:
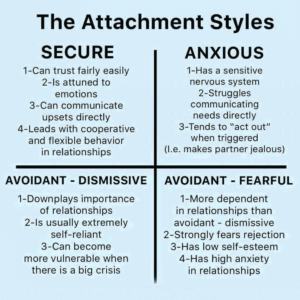
Anxious/Ambivalent- arising from an insecure environment where the child could not trust the caregiver. The child is constantly scanning the situation in case they are abandoned and/or constantly seek approval. They may also be emotionally dependent as adults.
Avoidant(dismissive)-arising from the child accepting their needs will not be met after experiencing lack of nurture, love, affection and significance. They may find relationships and feelings difficult to explore and avoid intimacy in relationships and find it very hard opening up at all later in life.
Avoidant (Fearful) also known as Disorganised which is a combination of the above two styles. Here, children display intense anger and rage eg being violent with other children or their toys. In adult life they tend towards anti -social behaviour types, avoiding relationships and/or easily explode in rages.
Coping with traumas
Dr. Arieh Shalev practiced at a major hospital in Jerusalem. At his hospital, when people are injured in a terrorist attack, he said the first thing his does is get the person’s family there. It sounds pretty basic advice, but other doctors would focus more on the treatment available and worry about calling the family later on. But he understood attachment theory- if the immediate family supports are there straight away, then there is less likelihood of escalating PTSD symptoms after the patient is discharged from hospital.
Resilience built on secure attachments
If the child had a secure attachment, they are generally more resilient when it comes to coping with a distressing event later in life. But if they did not have a secure attachment due to separation or neglect etc when they were a baby or very young, they may likely react differently to the same distressing event. This is why there can be different outcomes to the same distressing events between twins. One may bounce back when the other never recovers. They may have been treated differently by the main caregiver in their first few years of life. If they were both subject to the same abuse.
They may react differently and take different time frames to initially stop reacting. Add to that if one got comforted after the abuse happened and the other didn’t. The first trauma is the actual abuse. The secondary trauma is not having support. So many factors come into play when it comes to whether or not a distressing event (no matter how objectively small) will result in a trauma imprint.
The 4 main types of Attachment Profiles
There are generally 4 types of attachment styles according to the theory based on the infant or child’s exposure which are briefly illustrated here:
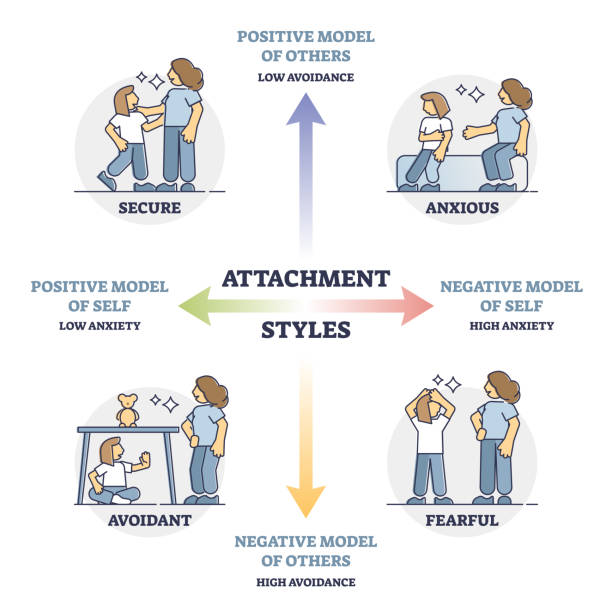
Operating from an attachment type
An “internal working model” of attachment is an imprint model. It’s not an indication of a problem inside of them , but rather a learned response to real-life events, to their actual relationship in their early days.
So from there, how you see yourself and how you see others will be influenced. Therefore, how you are able to interact with others and whether you are likely to have social anxiety for example will be impacted:
Healing with specific trauma therapy
Trauma has a profound impact on the body, the nervous system, and the brain. The autonomic nervous system is affected. Memory is affected. Negative beliefs held in the unconscious get structured and reinforced. Seemingly uncontrolled triggers develop. Destructive behaviors and bad feelings seem to flourish and go on auto pilot.
That’s why it’s so important to select a therapy that can reach those areas, not just the cognitive alert part of the mind we engage in by day to day talking. It doesn’t need to go as deep as hypnosis and it doesn’t need to retraumatize you by reliving past distressing events in detail.
Find out if TRTP is for you
More recent advances in therapy techniques such as TRTP are having amazing long term positive effects confirmed by audited studies. If you would like to know more about TRTP to help you overcome anxiety or depression or stress or PSTD, just book a complimentary call with me here: book a call. This is what my clients say about their results after receiving the TRTP therapy from me: testimonial